Introduction
Turner syndrome (TS) is a genetic syndrome related to partial or complete absence of one of the X chromosomes. Its incidence is one in 2500 female births. TS is associated with various physical morbidities: short stature, dysmorphic features, ovarian failure, cardiac defects, hearing difficulties, autoimmune diathesis. Subjects with TS also have various difficulties in cognitive and social skills.
Girls with TS entering adolescence need monitoring of medical problems that presented during childhood, screening for possible new comorbidities, and, on completion of growth hormone (GH) therapy, progressive adjustment of hormone replacement therapy (HRT). In this period of life, updated explanations, advice on lifestyle, and facilitation of autonomy in self-healthcare management are also mandatory.
International guidelines [1] strongly recommend the evaluation and addressing of psychosocial issues, by means of neuropsychological assessments at key transitional stages, and interventions for cognitive or psychological problems. With regard to the methodology, the counseling and therapeutic approach used in other young populations is generally accepted to meet the needs of girls with TS. Specific indications and literature on the treatment of psychosocial aspects are scarce[2] and mainly propose psychological assessment and group training where social skills are lacking.
Normal verbal function and IQ, but possible impairment of several non-verbal abilities with repercussions on executive function, characterize the neurocognitive profile of girls with TS. Visual-spatial processing, visual-motor capacity, visual attention and memory may be deficient, as may mathematical abilities, processing speed, abstract reasoning, the capacity to transform experience into stable learning, and the ability to sustain attention. Some patients with TS struggle with clustering concepts and with planning and organizing behaviors. Impairment of cognitive flexibility (i.e. the ability to switch between different concepts or to deal with unexpected conditions) is often present. If a non-verbal dysfunction is present, the recognition of emotions expressed by others (the perception of facial expressions, tone of voice, body language) may also be impaired, as may these subjects’ ability to identify and cope with their own emotions. On occasion, social impairment (social anxiety and poor assertiveness) may be demonstrated [3-7]. This cognitive pattern, influenced by genotype but always expressed with wide variability between individuals, is associated with, but not clearly related to, neuroimaging findings such as decreased gray matter volumes in the somatosensory, premotor, and parietal-occipital cortex, and increased volumes of the amygdala and orbital-frontal cortex [8]. The development of the brain in puberty, which is particularly vulnerable to genetic and hormonal influences, shows specific alterations [9].
Story of an ongoing project
A family and patient support organization (AFaDOC: Association of Families of Individuals with Growth Hormone Deficiency) has been active in Italy since 1993, providing expertise and advocacy for subjects with TS and their relatives. The association also provides psychological counseling, offering the first consultation free of charge for its members.
It is well known that peer influence is always a powerful factor in adolescent development and that peer group programs are a positive educational resource. Moreover, in subjects of every age affected by chronic conditions self-help groups constitute a structured avenue for improving adherence to treatment and quality of life [10]. In March 2014, the association organized its first residential group intervention for TS adolescents, led by a gynecologist and a psychologist, and focusing on sensitive topics for this age group. This initial small group intervention was based on the active methodology of the Standards for Sexuality Education in Europe [11,12]. Evidence demonstrates that un-targeted health promotion programs have several limits, whereas a learner-centered approach is crucial for the efficacy of all educational programs [13]. The first step was therefore to assess the needs of the target audience, using group techniques [14], i.e. specific activities, such as brainstorming or short surveys, aimed at identifying the difficulties they faced at school, within the family, with peers, or with medical treatments, and their help and support needs in this specific period of their lives. Gathering information in this unstructured manner allowed us, collectively, to draft a list of problems and priorities. During the pilot intervention the girls were involved in games and interactive activities designed to explore different relationships in their lives and the qualities they seek in close relationships, physical and mental changes already experienced and those they expected to experience, their help needs, and different ways of taking care of themselves.
Later we put a questionnaire to all the association’s adolescents, safeguarding the anonymity of participants, in order to better understand what information they needed as well as their perceptions of skill gaps in their everyday lives. They mainly asked for information about hormonal treatment, fertility and sexuality, and reported anxiety related to difficulties in relationships with peers, particularly in forming close friendships or intimate relationships. Impaired social functioning was the main reason for low self-esteem.
We subsequently structured the program to include the topics they suggested, and incorporate activities designed to explore feelings, emotions, characteristics of healthy relationships, and to improve verbal and non-verbal communication. The methodology was derived from that of life skills-based education programs for adolescents. In 1997, the WHO defined a core set of life skills necessary for the wellbeing of adolescents [15]: decision-making, problem solving, creative thinking, critical thinking, effective communication, interpersonal relationship skills, self-awareness, empathy, coping with emotions, and coping with stress. Skills-based health education programs require interactive and participatory learning methods [16] that allow participants (including the facilitators) to listen to and learn from each other: group discussion, brainstorming, educational games, situation analysis and storytelling with a subsequent debate. We proposed these activities to a slightly larger group during the AFaDOC Association Workshops. The qualitative evaluation of the experience, gathered at the end through participant interviews, revealed appreciation of both the content and the methodology.
Professionals involved in the project held a discussion in order to reformulate the objectives and to adjust the content to more specific outcomes; during this discussion, the consideration of a close link between cognitive profile and social functioning in girls with TS emerged. A reduced ability to interpret non-verbal social cues and recognize emotions, as well as executive dysfunction related to the loss of X-chromosome material, all play a role in the occurrence of social impairment [3, 6].
The coordinators of the program therefore decided to focus a part of the program mainly on visual-spatial orientation, using appropriate games and exercises and techniques from psychomotor practice [17]. Another focal point considered was the improvement of specific cognitive disabilities, such as difficulties in processing speed, abstract reasoning, and organization strategies [18]. The work on emotion recognition, and on interpretation of personal feelings and of the feelings and intentions of others people, through specifically designed activities or games [19, 20], remained a mandatory part of the curriculum.
The preliminary experiences and new proposals convinced the association to organize teen summer camps in holiday resorts, combining group activities with leisure time. One year later, a similar initiative was started with a pre-adolescent group, in this case focusing on physical development, psychosexual maturation, and related expectations and fears.
Considering our experience from a clinical point of view, it is to be noted that our groups included girls with different genotypes (complete monosomy, X deletions and mosaics), different phenotypes, at various stages of hormonal treatment (GH therapy, estrogen pubertal induction, or estradiol and progesterone replacement therapy), and with variable neurocognitive functioning. Independently of the wide inter-individual variability, many of our adolescents with TS have minimal neurocognitive impairment, most frequently in the visuospatial domain and in visual-motor coordination, but also poor facial and emotion recognition, and difficulties in non-verbal communication. The need for medical intervention for pubertal development and the delay in the attainment of sexual characteristics probably partially explain their shared perception of a barrier to reaching the adult female body and related expectations. Therefore, almost all these girls, faced with challenges concerning their femininity and integration into the adult world, need to improve in skills such as empathetic communication, decision-making, creativity and stress management. Together with individual psycho-therapeutic approaches, the AFaDOC teens’ group represented a safe space for active exploration of personal possibilities and limits and a friendly context for exchanges and learning.
The contents of the project were gradually expanded following input from the girls, but the facilitators also perceived their needs. Sometimes “missing topics” in discussions, such as sexuality or intimate perceptions, spoke more than direct requests.
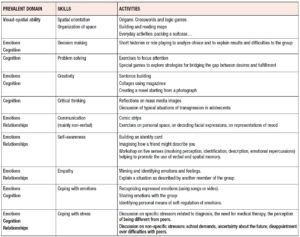
As regards the methodology of our meetings, we can trace its evolution over time. Starting from the original WHO definitions of life skills for adolescents [15], from a practical point of view, various aspects and competences were overlapping and could be aggregated into three domains: emotions, cognition, and relationships. The activities proposed to the group should cover and balance these different areas of learning and experience so as to help the participants deal with the demands and challenges of everyday life. Table 1 summarizes a few examples of methods and educational activities used in this context.
The work on impulsiveness, anxiety, and states of inhibition of thinking and action was a transverse feature across all the activities, as was improvement in awareness of personal capacities and limits, which serves as a foundation for interpersonal relationships and empathy.
The involvement, in the group project, of a teacher specialized in psychomotor practices made it possible to work more effectively on spatial orientation, representation and organization. The cooperation of a writer, an expert in reading and writing workshops, helped participants reach a turning point as regards their capacity for understanding and expressing personal feelings and reactions. Reading chosen passages of a novel, trying to perform or to mime single characters or situations, trying to concisely describe facts, emotions, behaviors, and their consequences and possible alternatives are all effective means of promoting intimate self-knowledge [21,22]. Exploration of the link between words and images, by working on the construction of “word-picture” activities, facilitates the organization of space and the discovery of a personal sense of esthetics. Techniques such as “blackout poetry” (taking a newspaper article and deleting all the words except those that the participants found suggestive or evocative, and then using these to compose a short poem) [23] work on self-awareness and creativity in an unprecedented way.
These expressive techniques are powerful instruments that, by enabling participants to focus on something apparently outside their lives, encourages them to lower their defense mechanisms and thus facilitates personal story telling, thereby providing an opportunity for self-narration very different from the “showcase” of social networks.
The presence in this context of a gynecologist/endocrinologist (the so-called medical corner) offered the adolescents with TS the possibility to ask questions or discuss clinical and therapeutic aspects of their lives, both individually and as a group, thus helping them to absorb the explanations and better understand their condition. It is well known that empathetic truth-telling supports positive integration of personal limits [24] and curbs anxiety. Reciprocal support improves acceptance of difficulties and, especially, enhances autonomy and self-care: the collective injection of GH in the evening is a small, but clear, example of this.
Based on our previous experiences, the current curriculum for pre-adolescents essentially consists of psycho-educational and psycho-motor activities mainly targeting visual-spatial and attentive deficiencies and aimed at regulating emotions and behaviors.
For adolescents, the proposal is to work chiefly on emotions, on awareness of feelings, of personal capacities and limits, and on creative possibilities as a foundation for interpersonal relationships and empathy.
Discussion
Our experience confirms the importance of association activities for patients with chronic diseases. The role of associations is to offer not only information but also interventions that can be considered mid-way between educational and therapeutic. This is especially true for subjects in transition between pediatric and adult healthcare, as the JAP study demonstrated [25]. In order to support participants better, the project needs to be tailored to specific physical and/or cognitive disabilities and needs related to the pathology. With the exception of the program of social skills group techniques (PEERS) validated for subjects with autism spectrum disorders and used for TS girls [26], there is little in the literature on specific group activities in TS.
After our five-year experience, the group continues to be a resource helping participants to overcome individual difficulties regarding acceptance of and motivation towards challenging (daily GH treatment) and long-term (HRT) treatments, and offering a space for debate and a training ground for raising awareness. Sometimes participation offers diagnostic benefits, bringing to light minimal deficiencies that parents or teachers had not recognized and in such cases it can be the starting point for short, individual psychological treatments. Conversation between the girls amplifies and maintains the mood of the summer camp experience, as do dedicated spaces set aside, for meetings, during annual association workshops.
The physiological turnover of the group is more of a resource than a limit, because it allows real-life experience to be handed on to younger girls. Joining the group is an important step towards growth. Nevertheless, leaving the group is also significant, because it means that the girls have almost concluded their personal transition into adulthood.
A limit of this experience is the still inadequate evaluation of the curriculum. Up to now, we have evaluated the results of the group work on the basis of the girls’ appreciation scale at the end of the camp and informal interviews with parents during annual meetings of the association. Given that the girls have different neuropsychological impairments and also a wide age range, it is not straightforward to build an assessment tool with clear indicators of the kind seen in sexuality education programs [27]. Our project is to study a test that explores the domains we described above, to be administered to pre-adolescent girls on entering the program and again after 2 and then 4 years of participation.
Another limit is that this activity is an under-utilized resource because, due to communication and logistical difficulties, the program has reached relatively few adolescents with TS. Promoting greater dissemination of information through pediatric endocrinology units and pediatric and adolescent gynecology services is our next step.
Disclosure/Conflict of interest
The involvement of professionals in the activities of the AFaDOC association is based on voluntary participation; this is also true of summer camp activities and for the organization of the programs. There is no conflict of interest.
Metella Dei and Roberta D’Aprile conceived and drafted the article. Cinzia Galasso
revised it. Gigliola Alvisi Palma Rossetti and Cinzia Sacchetti offered suggestions
and the final approval of the text.